Epidemiology, Transmission and Diagnosis
Epidemiology
KEY POINTS
- Genital herpes due to HSV-1 (often through facial to genital transmission) has become common. Therefore, HSV-1 is a common cause of primary genital herpes.
- Up to one in five adults are serologically positive for HSV-2, but most of these individuals will have asymptomatic or unrecognised disease.
- HSV-1 seroprevalence in the Australasian population is estimated to be about 80% in those older than 35 years.
- The natural history of genital HSV-1 infection shows significantly fewer recurrences and less subclinical shedding than genital HSV-2 infection.
- In New Zealand 53% of genital herpes lesions tested positive for HSV-1 in under 25 year olds. In the UK HSV-1 is the most common cause of genital herpes.
Natural history
Genital herpes is an infection caused by the herpes simplex virus (HSV) resulting in lesions on the genital area and nearby areas (i.e. buttocks, anal area and thighs).
There are two subtypes of HSV that can cause genital herpes, HSV type 1 (HSV-1) and HSV type 2 (HSV-2). Both are acquired from skin to skin contact - either oral to anogenital, or anogenital to anogenital. At the time of transmission HSV infects the genital epithelial cells and nerve endings. The virus uses retrograde axonal transport to establish persistent infection in the sacral ganglia. Some time after transmission, classically 2-14 days later, the patient may have their first initial episode. However many people who are HSV positive do not have any symptoms, or, have their first episode months to years later; many individuals are asymptomatic or have very mild symptoms after initial exposure, which may go unnoticed. Later, due to triggers such as stress, illness, or hormonal changes, the virus can reactivate, causing the first noticeable outbreak. In the primary episode the severity of symptoms differs markedly between individuals, but lesions can last up to 3 weeks in severe cases. HSV can be periodically reactivated, and the virus will travel down the axon to skin and mucosal surfaces, where viral shedding may be associated with genital ulcers or, more commonly, is asymptomatic. Therefore, the majority of genital herpes are likely to be acquired subclinically. If a recurrence is symptomatic, the lesions are not as severe as the primary episode and may take 3-7 days to heal.1 In a reactivation HSV can be shed from the site of initial transmission i.e. from the external genitalia, the anorectum, the cervix, and the urethra.
Epidemiology of HSV-1
A 2023 meta analysis showed 80% of the Australian population is seropositive for HSV-1, a higher level than that observed in other Western countries.2 Seropositivity does not determine the site of infection but available data suggests that HSV-1 accounts for 35% of confirmed anogenital infections in Australia,3 and a Waikato-wide study found that 30–40% of anogenital isolates annually were due to HSV-1.4 The Waikato data also reported that HSV-1 accounted for 53% of positive isolates from individuals aged under 25 years, 30% of isolated in those aged 25–35 years, and 26% of isolates in those aged >35 years. The seroprevalence of HSV-1 (like that of HSV-2) increases as age increases, and tends to be more common in women than in men.5
Routine typing of isolates enhances a clinician's ability to provide prognostic information and optimal clinical care. Given that a substantial proportion of individuals with genital herpes will be infected with HSV-1, it is no longer accurate to assume that genital herpes is due to HSV-2 infection.6 In the UK, genital herpes is more likely to be due to HSV-1 rather than HSV-2.7 The natural history of genital HSV-1 infection shows significantly fewer recurrences and much less subclinical shedding than genital HSV-2 infection.6, 8 A prospective cohort study showed genital shedding was frequent after first-episode genital HSV-1, particularly amongst those with primary infection, and declined rapidly in the first year of infection. 30% of people who have an HSV-1 initial episode anogenitally will not experience a recurrence in the first year after their initial episode.9 In summary, genital HSV-1 recurs infrequently, if at all, for most patients, with recurrence rates continuing to decline in the years following the initial infection.
Prior genital HSV-1 infection does not alter the risk of subsequent HSV-2 infection, although rare, if acquired the HSV-2 has increased odds of being asymptomatic.10
Epidemiology of HSV-2
HSV-2 prevalence varies between countries and, depending on the demographics of the population being tested.11 One consistent finding across countries is that, although the incidence of new infections is highest in young adults, the fact that infection is lifelong means that the overall seroprevalence of HSV-2 increases with age.11 Participants in the Dunedin Multidisciplinary Health and Development cohort study provided serum for HSV-2 antibody status at the ages of 21, 26, 32 and 38 years.12 By the age of 38 years, 26.8% of women had been positive for HSV-2 compared with 17.3% of men, indicating a higher biological susceptibility to infection in women.12 The rate of new HSV-2 infection was highest at age 21–26 years for women and 26–32 years for men, then declined with age, consistent with decreasing infectivity of long-term prevalent infections.12
Only one-third of individuals appear to develop symptoms at the time of acquisition of infection with HSV-2.10 Approximately 20% of people that are serologically positive for HSV-2 have been diagnosed as having genital herpes, most people with HSV-2 are asymptomatic or don't recognise their symptoms as genital herpes.10 Individuals with HSV-2 will, on average, experience approximately four clinical recurrences a year.13
Transmission
KEY POINTS
- Transmission occurs during oral to genital, or genital to genital skin-to-skin contact with an individual who is shedding the HSV-1 or HSV-2 virus.
- HSV-1 is commonly transmitted through facial to anogenital contact. However, it can be transmitted anogenital to anogenital contact.
- HSV-2 is mainly transmitted through anogenital to anogenital contact.
- Virus shedding occurs during symptomatic recurrences. Skin to skin contact with the affected area should be avoided during this time.
- Asymptomatic shedding can occur a small percentage of the time between recurrences, and from individuals who are unaware that they have HSV because they are asymptomatic.
Most HSV-1 or HSV-2 infections are acquired from an individual who is shedding virus but unaware that they are infected because they are asymptomatic or have only mild symptoms.8 HSV is transmitted during direct skin to skin contact through a break in the skin or mucous membranes. For genital infections, this is usually during sexual contact. It is more likely when there are lesions present (e.g. vesicles or ulcers), and happens most often from men to women. Therefore, sexual contact should be avoided when active lesions are present.
HSV is inactivated at room temperature and by drying. Therefore, non-contact spread (e.g. via inanimate objects) is considered unlikely. Autoinoculation resulting in spread to different anatomical sites can occur (e.g. facial, whitlow), although this is believed to be uncommon. GRADE C
Asymptomatic viral shedding
HSV intermittently sheds virus in the absence of symptoms, which is why sexual transmission can occur during asymptomatic periods. These intermittent episodes of asymptomatic viral shedding are more frequent in the following situations:
- With genital HSV-2 versus genital HSV-1 infection.
- During the first 12 months after acquiring HSV.
- In those with more frequent symptomatic episodes.
- Within a week before or after a symptomatic episode.
- In those who also have HIV infection.
The viral load threshold for transmission from an episode of asymptomatic shedding has not been established. It is impossible to be certain when asymptomatic viral shedding occurs for a given individual, but it is important that infected individuals understand that they are not infectious all the time.
Most people who have genital HSV are unaware they have it as their symptoms are so mild they aren't diagnosed or they have no symptoms. This cohort also sheds asymptomatically.
Reducing transmission risk
KEY POINTS
- Consistent condom use reduces, but does not eliminate, the risk of HSV transmission.
- Sexual contact with the active area should be avoided when facial or anogenital lesions are present.
- Suppressive oral antiviral treatment will significantly reduce, but not eliminate, the risk of transmission.
Barrier methods
Although helpful, male and female condoms do not provide complete protection against the transmission of HSV because they do not cover all affected areas, could slip or break, and because close genital contact or contact with infectious secretions may occur during foreplay.14 Nevertheless, consistent condom use offers moderate protection against HSV infection in both men and women.15 Male condoms, used at least 25-60% of the time, reduce the rate of transmission of HSV-2 by 50%.16
GRADE B Data on ability of male condoms to prevent male-to-male transmission, and on the efficacy of female condoms, are lacking. Condom use should be tailored to the individual circumstances.
Oral - genital contact
People who do not acquire HSV-1 during childhood are at risk of HSV-1 at any site, including genital infection, during adulthood. Transmission may occur whilst receiving oral sex from someone who has facial HSV-1, even if the source partner is asymptomatic. It is estimated that up to one-third of individuals who are HSV-1 antibody positive do not have a clinical diagnosis of facial herpes,17 but will still shed HSV-1 virus.18 Whilst a prior facial HSV-1 infection can provide some immune response, it does not fully protect an individual against genital HSV-1. It may reduce the severity of symptoms if genital HSV-1 is contracted, but it does not prevent infection altogether. Facial HSV-2 in isolation is uncommon. Oral-genital contact should be avoided when facial lesions are present. GRADE C
Antivirals
Aciclovir, valaciclovir and famciclovir all suppress symptomatic and asymptomatic shedding of HSV by 80–95% (famciclovir is not subsidised or marketed in New Zealand, but is available in pharmacies).19 Valaciclovir has been shown to be more effective than famciclovir in reducing viral shedding and transmission.20 It has also been shown that suppressive treatment with once-daily valaciclovir reduces transmission to the discordant partner by 48% for HSV infection acquisition and by 75% for clinical symptomatic genital herpes.13 The antiviral medications for the treatment and suppression of genital herpes are generic and cheap. The Pharmac website shows that currently (2024) a month of valaciclovir 500mg once a day for 30 days costs $9.64 whilst a month of suppressive aciclovir is $6.23.
Co-infection
Co-infection can occur. Pre-existing genital HSV-1 infection does not appear to decrease the risk of being infected with genital HSV-2, but does increase the likelihood that the HSV-2 infection will be asymptomatic.10 If genital HSV-2 is acquired first, then a new HSV-1 genital infection does not affect the frequency of HSV-2 recurrences.
Diagnostic Tests
KEY POINTS
- Suspected genital herpes should be confirmed by a nucleic acid amplification test (NAAT) such as polymerase chain reaction (PCR).
- PCR is the best test in Aotearoa New Zealand for the diagnosis of active HSV lesions.
- A negative result does not rule out HSV infection.
- HSV serology is not recommended.
Clinical diagnosis of HSV infection is inaccurate, with a 20% false positive rate.10 Therefore, suspected genital herpes must be confirmed by viral swab PCR. Recurrent lesions, which have not been previously confirmed, should also undergo PCR testing for HSV. Detection of HSV DNA by PCR in the lesion establishes the diagnosis and provides viral typing. However, the results of PCR testing are dependent on multiple factors, including the adequacy of the specimen collected from a viral swab and the time delay between onset of symptoms and presentation. Therefore, a negative PCR test result may not exclude HSV infection because the method is dependent on adequate sample collection. As a result, it is important not to delay appropriate therapy whilst waiting for the results of diagnostic testing.
Serology
HSV-1 and HSV-2 serology is not recommended except in rare, specific situations. The interpretation of HSV serology is difficult and seldom gives clinically relevant information.
Serology is not recommended for the following reasons:
- HSV IgG positivity shows infection with HSV-1 or HSV-2 in the past.
- HSV-1 and HSV-2 seroconversion can occur sometime following the initial exposure. Some people seroconvert in 2–6 weeks, but others take longer (months) and some may not seroconvert. In addition, reversal from seropositive to seronegative status may occur if there is minimal antigenic stimulation.
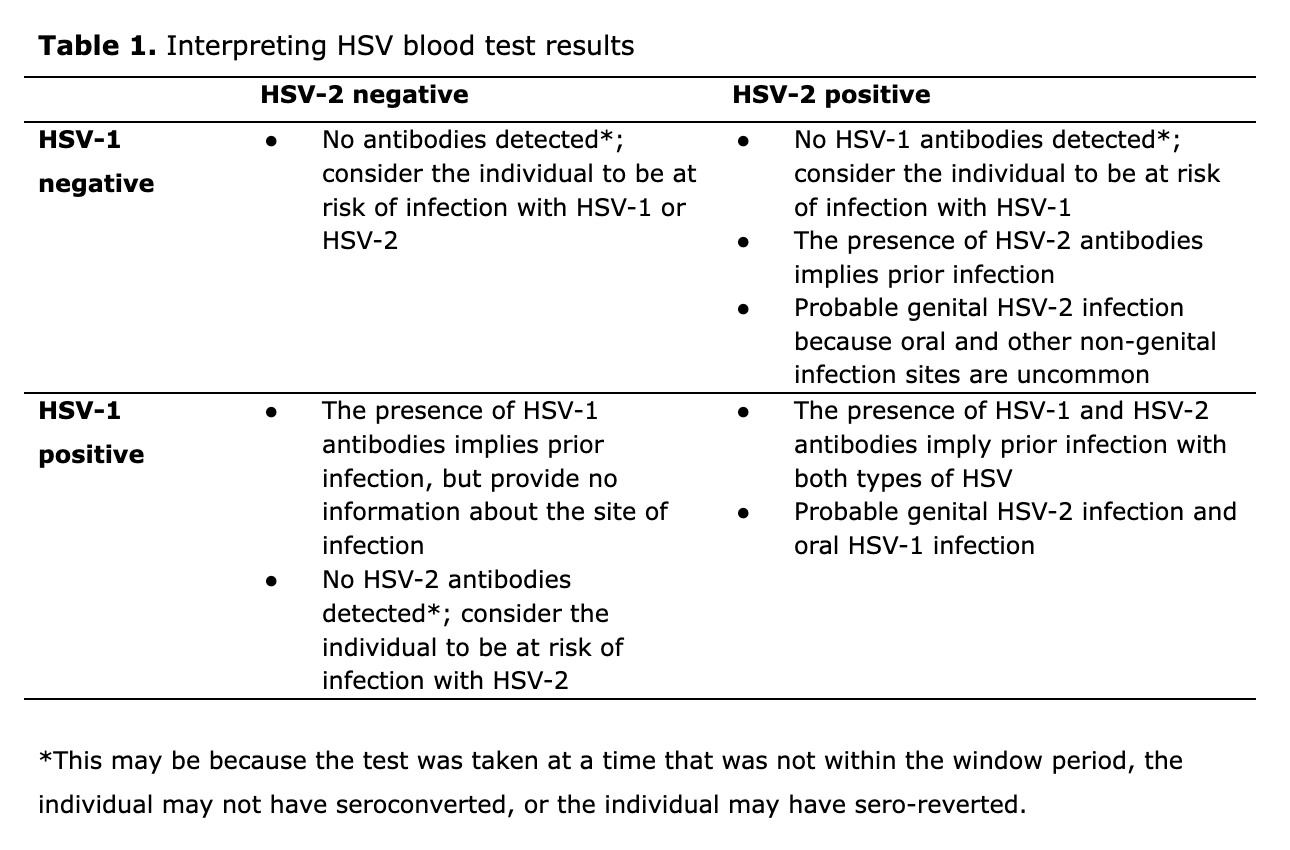
- Serology does not distinguish the anatomical site of infection (see Table 1).
- Even highly sensitive and specific assays have poor predictive values in low prevalence populations.
- HSV-2 antibodies are very likely to indicate genital herpes. HSV-1 antibodies do not differentiate between genital and oropharyngeal infection.
- Many commercial tests do not give type specific information so have no value as are herpes urine tests. Commercial tests often have differing sensitivity for HSV-1 and HSV-2 and different ethnic groups.
- Commercial point of care (POC) tests available online are not supported for the diagnosis of HSV-2. They are not reliable and should not be used.
- Western blot is the diagnostic gold-standard but it isn't widely available and is cost prohibitive.
- Genital herpes screening is not recommended and is likely to be more harmful than helpful.
Serology may be helpful in the following situations:
- Recurrent genital disease of unknown cause.
- Counselling pregnant patients, serology can be helpful to determine whether the current infection is primary (potentially with viremia and therefore a higher risk of transmission) or a recurrence (much lower transmission risk, (see also the Genital Herpes in Pregnancy chapter).
- Investigating and advising an asymptomatic pregnant partner or possible discordant couples planning pregnancy who are concerned about possible transmission in pregnancy.
Education, rather than serological testing, is recommended for most partners of HSV-positive individuals due to the possibility of false positive/false negative serology results.
Key information to discuss with a patient who asks for a blood test includes the following:
- Explain that serology is not accurate enough to be used as a test for herpes because there is reasonable risk of a false negative or and false positive result.
- Some people take a long time to develop antibodies to HSV and some people don't develop antibodies at all.
- A blood test does not tell you the anatomical site of the infection.
- If you have any questions about the relevance of a serological test you can reach out to a sexual health specialist for advice.
References
- Corey L, Adams HG, Brown ZA, Holmes KK. Genital herpes simplex virus infections: clinical manifestations, course, and complications. Ann Intern Med 1983; 98 (6): 958–972.
- AlMukdad S, Harfouche M, Farooqui US, et al. Epidemiology of herpes simplex virus type 1 and genital herpes in Australia and New Zealand: systematic review, meta-analyses and meta-regressions. Epidemiol Infect 2023; Feb 8: 151: e33.
- Haddow LJ, Dave B, Mindel A, et al. Increase in rates of herpes simplex virus type 1 as a cause of anogenital herpes in western Sydney, Australia, between 1979 and 2003. Sex Transm Infect 2006; 82 (3): 255-9.
- Gray E, Morgan J, Lindeman J. Herpes simplex type 1 versus Herpes simplex type 2 in anogenital herpes; a 10 year study from the Waikato region of New Zealand. NZ Med J 2008; 121 (1271): 43-50.
- Nguyen N, Burkhart CN, Burkhart CG. Identifying potential pitfalls in conventional herpes simplex virus management. Int J Dermatol 2010; 49 (9): 987-93.
- Corey L, McCutchan JA, Ronald AR, Handsfield HH. Evaluation of new anti-infective drugs for the treatment of genital infections due to herpes simplex virus. Infectious Diseases Society of America and the Food and Drug Administration. Clin Infect Dis 1992; 15 (Suppl 1): S99-107.
- Scoular A, Norrie J, Gillespie G, et al. Longitudinal study of genital infection by herpes simplex virus type 1 in western Scotland over 15 years. BMJ 2002; 324 (7350): 1366–1367.
- Wald A. Herpes simplex virus type 2 transmission: risk factors and virus shedding. Herpes 2004; 11 (Suppl 3): 130a-7a.
- Johnston C, Magaret A, Son H, et al. Viral Shedding 1 Year Following First-Episode Genital HSV-1 Infection. JAMA 2022; 328 (17): 1730–1739.
- Langenberg A, Corey L, Ashley R, et al. A prospective study of new infections with herpes simplex virus type 1 and type 2. N Engl J Med 1999; 341 (19): 1432–1438.
- Looker KJ, Garnett GP, Schmid GP. An estimate of the global prevalence and incidence of herpes simplex virus type 2 infection. Bull World Health Organ 2008; 86 (10): 805-12, a.
- Dickson N, Righarts A, van Roode T, et al. HSV-2 incidence by sex over four age periods to age 38 in a birth cohort. Sex Transm Infect 2014; 90 (3): 243-5.
- Benedetti J, Corey L, Ashley R. Recurrence rates in genital herpes after symptomatic first-episode infection. Ann Intern Med 1994; 121 (11): 847–854.
- Langenberg A. Interrupting herpes simplex virus type 2 transmission: the role of condoms and microbicides. Herpes 2004; 11 (Suppl 3): 147a-54a.
- Wald A, Langenberg AG, Krantz E, et al. The relationship between condom use and herpes simplex virus acquisition. Ann Intern Med 2005; 143 (10): 707-13.
- Martin ET, Krantz E, Gottlieb SL, et al. A pooled analysis of the effect of condoms in preventing HSV-2 acquisition. Arch Intern Med 2009; 169 (13): 1233–1240.
- Cowan FM, Johnson AM, Ashley R, et al. Relationship between antibodies to herpes simplex virus (HSV) and symptoms of HSV infection. J Infect Dis 1996; 174 (3): 470-5.
- da Silva LM, Guimarães AL, Victória JM, et al. Herpes simplex virus type 1 shedding in the oral cavity of seropositive patients. Oral Dis 2005; 11 (1): 13-6.
- Wald A, Corey L, Cone R, et al. Frequent genital herpes simplex virus 2 shedding in immunocompetent women. Effect of acyclovir treatment. J Clin Invest 1997; 99 (5): 1092-7.
- Wald A, Selke S, Warren T, et al. Comparative efficacy of famciclovir and valacyclovir for suppression of recurrent genital herpes and viral shedding. Sex Transm Dis 2006; 33 (9): 529–533.